

Julia Nogueira Marx Gonzaga1; Luciene Chaves Fernandes2
DOI: 10.17545/eOftalmo/2025.0016
ABSTRACT
Clinical assessment forms the basis of visual rehabilitation (VR) planning, guiding interventions and the prescription of assistive technologies to maximize the functionality of patients with vision impairment. Clinical assessment comprises a detailed anamnesis and specific ophthalmic examination to understand the patient's ocular history, systemic conditions, emotional impact of visual loss, expectations, and goals, and to strengthen the doctor/patient/family relationship. The assessment of visual functions allows for estimating the functional response and guiding individualized treatment strategies. Careful refraction examination is essential because proper correction of refractive errors significantly improves residual vision and, in some cases, is the main intervention. A complete ophthalmic examination complements the diagnosis and supports clinical or surgical decisions. The patient-centered, realistic, and personalized approach is the core of visual rehabilitation, conditioning the success of the rehabilitation process and aiming to promote autonomy, educational and socio-cultural inclusion, and better quality of life.
Keywords: Vision impairment; Visual rehabilitation; Ophthalmic evaluation; Visual function; Assistive technologies.
RESUMO
A avaliação clínica constitui a base do planejamento em reabilitação visual, orientando intervenções e prescrição de tecnologias assistivas para maximizar a funcionalidade do paciente com deficiência visual. Consiste de anamnese detalhada e exame oftalmológico específico de modo a compreender a história ocular, condições sistêmicas, impacto emocional da perda visual, expectativas e objetivos do paciente, além de fortalecer a relação médico–paciente–família. A avaliação das funções visuais permite estimar a resposta funcional e direcionar estratégias terapêuticas individualizadas. O exame refracional cuidadoso é fundamental, pois a correção adequada de ametropias pode melhorar significativamente a visão residual e, em alguns casos, ser a principal intervenção necessária. O exame oftalmológico completo complementa o diagnóstico e subsidia decisões clínicas ou cirúrgicas. A abordagem centrada no paciente, realista e personalizada, é o núcleo da reabilitação visual e condiciona o sucesso do processo reabilitador, visando promover autonomia, inclusão educacional e sociocultural e melhor qualidade de vida.
Palavras-chave: Deficiência visual; Reabilitação visual; Avaliação oftalmológica; Função visual; Tecnologias assistivas.
INTRODUCTION
Clinical assessment is essential for planning the visual rehabilitation (VR) program as it guides treatments, interventions, and the prescription of assistive technologies.
The rehabilitation of patients with vision impairment involves multidisciplinary and interdisciplinary action and usually includes ophthalmologists, occupational therapists, physiotherapists, speech therapists, specialized educators, mobility guides, and psychologists who all collaborate to promote the maximum use of residual vision and other sensory and cognitive resources available. The central objective is to improve the patient's functionality to allow school, social, economic, and cultural inclusion; provide independence; and improve the quality of life. To achieve this goal, a complete ophthalmic assessment is required, which comprises the following: clinical history, assessment of visual functions, complete ophthalmic examination, calculation for magnification, and adaptation of optical, non-optical, electronic devices. Each stage contributes to the construction of an individualized and realistic treatment plan, which is fundamental to the success of VR1-5.
OPHTHALMIC ASSESSMENT
1. Clinical history / Anamnesis
Anamnesis is one of the pillars of the VR process and directly impacts the success of the interventions. It starts from the first contact with the patient, when posture, behavior, attention to external stimuli, exploration of the environment, and mastery of movement in an unfamiliar space are observed. These initial observations already provide important clues about the degree of visual impairment and how the patient uses their residual vision1,3,4.
A series of carefully selected questions is then asked, and the answers inform the doctor about the degree of visual impairment, the patient's understanding of their diagnosis, expectations for the examination, and prescription. The anamnesis should include information about the ocular disease, namely its onset and progression, received treatments, patient's comorbidities that may contribute to visual worsening or that impact VR (such as tremors, hypoacusis, cognitive impairment, reduced mobility, changes in balance, etc.), medications in use, visual difficulties and their progression over time, predominantly affected eye, and family history of vision impairment. The presence of mood changes related to visual loss, experience of visual hallucinations (Charles Bonnet Syndrome), expectations and fear about visual threat, worsening of the condition, and loss of autonomy should also be investigated1,6.
It is crucial at this point to establish a doctor/patient/family relationship of trust, acceptance, respect, and safety. Clarity about the purpose of VR is essential so as not to create unrealistic expectations: it doesn't restore lost vision but improves functional response significantly. Thus, the patient should work within real expectations and not wait for a miraculous response1,5.
The aim is to get to know the patient's goals and identify areas of interest, their activities before visual impairment (VI), the duration and progression of visual loss, knowledge and previous experience with optical/electronic resources, and the patient's and their family's ability to cope with the disability, according to each case. As Gilbert points out: "When assessing a person with vision impairment, it is very important to find out what they can and cannot do, what their most annoying symptoms are, and what activities they want to continue"7,8.
Careful investigation of the patient's life, expectations, and concerns regarding treatment is of great importance. Reactions to visual loss are variable, often unpredictable or surprising, and change over time. The level of threat, insecurity, fear of the future, conflicting emotions, sadness and depression are all feelings that patients and family members bring into the consultation room. In this context, the importance of the doctor/patient/family relationship in promoting VR is evident.
Factors such as motivation, interest, age, schooling, autonomy in activities of daily living, systemic conditions, acceptance of the disability, and the extent of the eye injury also need to be included in the assessment. Based on these elements, strategies are built jointly with the patient and their family while respecting their limitations and goals. The success of VR depends on the active participation of everyone involved1,8.
2. Visual functions
Visual functions comprise sensory abilities related to the perception of light and shape, recognition of details, size and shape discrimination, color perception, interpretation of visual stimuli, and determination of a functional response. Visual acuity (VA), visual field (VF), contrast sensitivity (CS), glare, color vision, binocularity, ocular motility, and other functions specific to each case should be considered1-3.
This article addresses VA, VF, and CS measurements, which are essential for understanding the functionality of vision and for individualized prescription of aids.
2.1 Visual acuity (VA)
VA refers to the ability of the visual system to distinguish details in high contrast. It is defined as the smallest retinal image that can be perceived clearly at a given distance. Although it is an essential quantitative measure, in isolation, it does not determine an individual's functional performance1,3,9,10.
During the assessment, efforts should be made to obtain a reading of an optotype by adjusting the distance and positioning of the table according to the residual VF. It is important for classifying visual impairment and thus make a proper calculation of the necessary magnification(1). VA should be measured for distance and near vision, monocular and binocular vision, with and without correction. In general, binocular VA is 5%–10% better than monocular VA1,3,11.
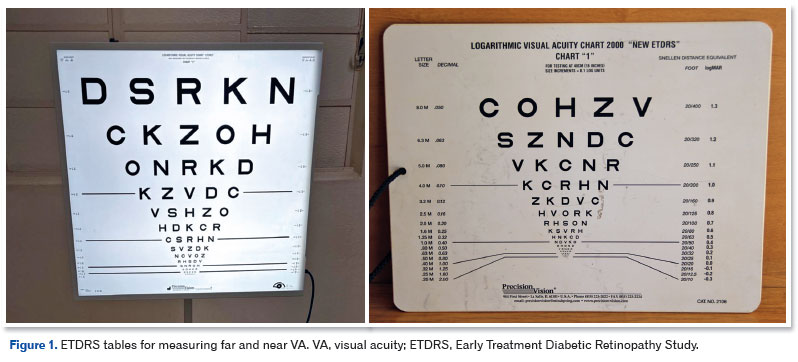
The tables used for measuring must be appropriate for the individual's age, abilities, and level of understanding. The World Health Organization (2015) recommends using the Lea Hyvärinen (LH) table for illiterate people and the Early Treatment Diabetic Retinopathy Study (ETDRS) table for literate people. Teller cards can be used if the patient cannot respond to the other tests2. The finger count test should be avoided because it is not standardized (Figure 1).
During the examination, it is important to observe the patient's behavior when reporting the optotypes: "the patient looks at the scotoma" (Fletcher)10. If the patient does not inform one side of the table, a scotoma may be present at that site; rapid movement of the eye or head while reading the table signals a large central scotoma with poor localization of eccentric vision, and improved reading speed with good lighting may indicate relative scotoma10. A patient who has difficulty identifying large optotypes but performs better with smaller ones may have an annular scotoma or a small residual central island of vision; this is often seen in cases with extensive peripheral field constriction and can severely impair reading1,3,10.
Reading ability is a standard measure of functional vision and guides the choice of the optical/electronic aid to be prescribed, as well as its magnification. It is measured by reading acuity (the smallest print size a person can read without making errors) and reading speed (words/min). It is considered that the speed of 80 words/min enables fluent, rapid reading, and the speed of 40 words/min allows directed, focused reading12.
AV-based prognosis
• AV up to 20/200 (0.1): Optical resources are of low magnification power, at a comfortable focal length (up to 10 cm), in a binocular prescription, which reduces the effect of scotoma and improves AV in addition to increasing VF and contrast. Better functional performance.
• AV between 20/250 (0.08) and 20/400 (0.05): Monocular prescription; short focal length (7–5 cm). Motivation and educational training for the functional use of the proposed aid are important to achieve success.
• AV less than 20/400 (0.05): Severe difficulty. Video magnification is a good idea.
• AV < 20/800 (0.025): Reserved prognosis. Video magnification is a must. Consider Braille, orientation and mobility, and replacement aids1,10,13.
2.2 Visual field (VF)
VF is defined as the total area that can be perceived while maintaining a fixed gaze (ICF-2003)14. It reveals the ability to simultaneously perceive visual information from various parts of the environment, and thus measures central and peripheral visual function. Evaluation of the VF is essential for diagnosing the disease and monitoring its progress, classifying visual impairment, and selecting the optical and electronic resources to be prescribed1,3,10,11.
The assessment is made using manual or automated perimeters or, more recently, microperimetry, which is more accurate for scotometry4,13,15,16. VF measurement includes the assessment of scotomas and fixation. Fixation can be foveal or eccentric, stable or unstable. The eccentric area of the retina usually used for fixation is referred to as the Preferred Retinal Locus (PRL). Although research into fixation and the PRL is ongoing, it is suggested that eccentric fixation is a dynamic process wherein patients use multiple retinal foci and that fixation changes according to the task, the size of the print, and the lighting. VF assessment using traditional automated perimeters is less accurate in patients with unstable or non-foveal fixation due to macular disease. In these cases, microperimetry is more suitable for assessing fixation and scotomas, thanks to eye-tracking technologies and simultaneous retinal images with the visual stimulus. Macular microperimetry evaluates the central VF monocularly. Some brands offer the option of training with biofeedback or fixation training with a PRL4,13,16.
Scotomas can also be assessed using non-automated methods such as manual perimeters, macular perimetry, an Amsler grid, and other subjective tests such as confrontation field, disc perimeter, and tangent screen. These non-automated tests can be performed binocularly to provide useful information on the patient's fixation while using binocular vision.
In a functional approach, the most frequent situations relating to the VF are considered3.
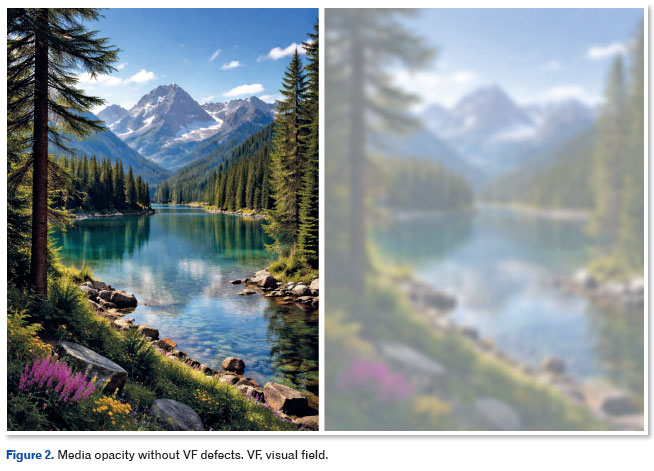
A. Opacity of media without a VF defect
It occurs in cases with corneal opacities, cataracts (especially posterior subcapsular cataracts), inflammation, and vitreoretinal hemorrhage. It creates VA reduction, blurry image, poor contrast response, and glare. The response to magnification is limited, given the enlargement of an already deteriorated image. Attention should be paid to correcting existing ametropia with the aim of improving the quality of the image to be enlarged. You should use the minimum magnification necessary for the optical aids, and using video magnifier is a good option, especially in reverse polarity text (black background/white letters). Non-optical resources to increase contrast and reduce glare are widely used to improve the functional response1,3,10 We highlight the efficiency of yellow filters for indoor or low-light environments and amber filters for higher light environments, with an associated polarized filter to reduce light dispersion. Other resources to consider include a typescope, high-contrast materials in daily activities, black ink on white paper, and wearing a cap or a visor (Figure 2).
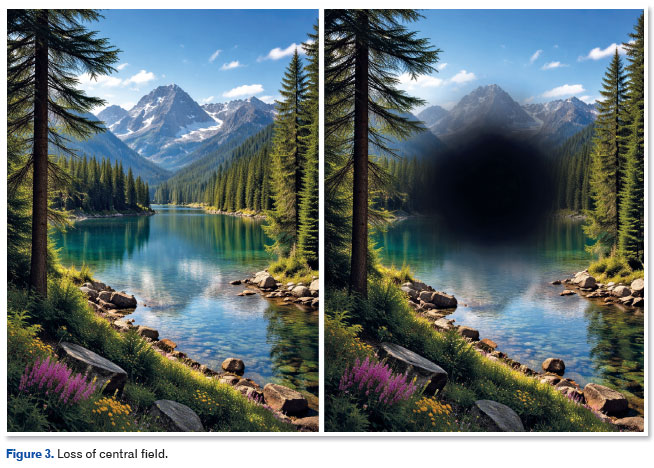
B. Loss of central field
It is the most prevalent defect in low vision, affecting around 83% of patients referred for VR(11). It occurs in cases with degenerative, inflammatory, toxic, vascular, or dystrophic diseases, such as Stargardt's disease, toxoplasmic retinochoroiditis, and age-related macular degeneration (Figure 3).
Scotomas vary in density and location according to the form of presentation and stage of the disease. Binocular vision reduces the impact of scotomas and, consequently, there is a better functional response, except when the dominant eye has the largest scotoma1,5,10.
The functional impact on daily activities is profound, especially when it comes to reading and recognizing faces. Low contrast sensitivity, glare, metamorphopsia, and dyschromatopsia may be present and hinder the functional response. The ability to read becomes limited when there is a scotoma in the area of fixation or to its right, and the prognosis is better when the scotoma is located above fixation. It is important that patients are aware of scotomas and know how to avoid them.
Appropriate educational strategies encourage the search for a new fixation point and, consequently, better visual performance for reading. Educational training in eccentric fixation may be necessary before prescribing optical and electronic resources5,10. Magnifying the retinal image, increasing contrast, and adjusting the lighting are also assertive VR strategies in these cases.
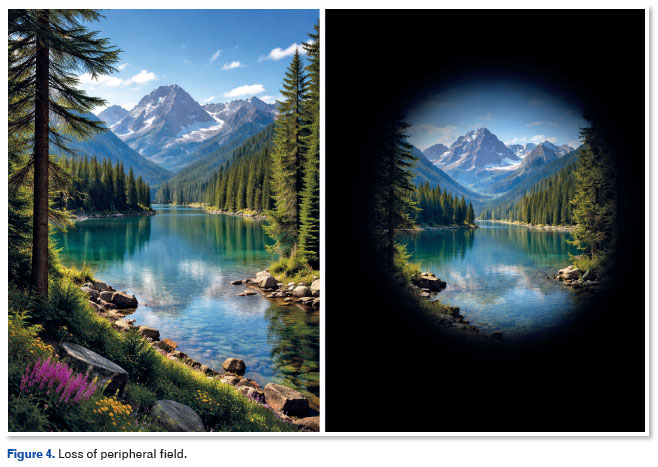
C. Peripheral field loss
It occurs in cases with dystrophic, inflammatory, and vascular conditions, with retinitis pigmentosa (RP), glaucoma, and diabetic retinopathy (DR) being the most common3. Peripheral vision is essential for spatial orientation and awareness of obstacles. When there is peripheral VF loss, vision worsens at night and in low-light areas, making movement and light/dark adaptation difficult (Figure 4).
The patient should be instructed to perform activities in daylight and be referred for orientation and mobility when necessary. Peripheral involvement can be localized, corresponding to laser photocoagulation scars in the DR, or diffuse. Central field loss may be associated with a significant reduction in contrast response.
In cases where the loss occurs gradually, the individuals develop unconscious compensation mechanisms to scan the environment through eye and head movements.
Unlike central field loss, difficulty in reading is not a primary complaint because a field only 10º in diameter allows normal or almost normal reading if VA is normal.
It is important to correct the existing ametropia. To allow the use of the residual VF, image scanning can be considered, being the most widely accepted method and yielding the best functional results. Image minification can be achieved using a reverse telescope, negative lenses, or VF expanders such as prism lenses for localized VF loss or VF expander telescopes such as the Ocutech, Design for vision and Walters telescopes, which are discussed in another chapter. A greater difficulty in responding to optical aids is expected, especially if the VF is smaller than 10º, at which point a hand-held magnifier and a video magnifiers become the most appropriate choice. Glasses are well accepted, with minor additions. Consider yellow filters for indoors and gray or amber filters for outdoors. In conditions with peripheral field loss, orientation and mobility are greatly compromised. For VA ≤ 20/800 (0.025) or VF of 10º or less, the use of a cane or a guide dog is required1,3,10,11. In advanced cases, non-visual aids should be considered.
2.3 Contrast sensitivity (CS)
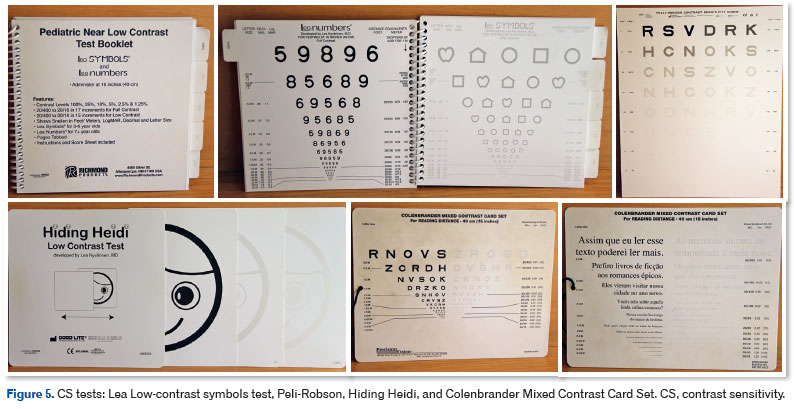
It is the visual function related to the ability to differentiate between an object and its background using the minimum amount of lighting (CIF, 2003)14. It is a psychophysical parameter that helps analyze the quality of vision and assess the overall visual response, involving the optical and neural systems. CS has been considered more important than VA in terms of the functional response of vision1,3,10,11. Most of an individual's daily activities are performed in low-contrast situations, so the investigation of VA combined with the study of CS provides a more comprehensive picture of the patient's functionality11. Despite the importance of CS, the equipment needed to determine its value is not always available in the ophthalmologists' consultation rooms. Other options for evaluating CS include sinusoidal grid tests (e.g., VCTS6500, FACT, Arden Grids, etc.) and tests with letters or pictures (e.g., Hiding Heidi, Peli-Robson, Lea low-contrast symbols tests, etc.) (Figure 5)1,2.
Patients with a low response to contrast often experience significant limitations in their daily activities. They complain of blurred or hazy vision, difficulty recognizing faces and walking down stairs, and reduced reading speed (30%)1,10,11.
A deficit at low spatial frequencies is a negative indicator for mobility, and a deficit across all frequencies leads to greater impairment of visual performance1,10,11.
Knowing the response to contrast is essential in the event of an unfavorable response to magnification3. It supports orientation in daily activities and the preparation of materials suitable for VR. The binocular response provides an improvement of up to 42% compared to the monocular response (binocular summation), which leads to opting for a binocular prescription whenever possible1,10,11. Low contrast requires better lighting, higher magnification, and the use of yellow and amber filter lenses1,11. A very low response to contrast makes it difficult to adapt to the optical aid. Moya et al.17 observed a better response to the adaptation of optical aids in cases where there was a better response at low spatial frequencies.
Other visual functions such as color vision, glare, adaptation to light and dark, ocular motility, and stereopsis must also be considered for each case.
3. Examination of refraction
Uncorrected refractive errors stand out as the leading cause of DV worldwide (49%), representing the main cause of moderate and severe DV (53%) and the second leading cause of blindness. It is the first cause of visual loss among children (63%), and high myopia has become one of the main causes of irreversible vision loss in the world18. Therefore, a thorough examination of refraction is essential when assessing low vision because the necessary magnification is calculated based on properly corrected VA. Better VA, VF, and CS are achieved with adequate refraction. In addition, uncorrected refractive errors contribute to the worsening of existing low vision.
Sunness et al.16 analyzed corrected VA in a population with low vision and observed that 11% of all patients gained two or more lines of VA, 3% of patients gained four or more lines, and, in 18% of patients, the worse-seeing eye became the better-seeing eye after optical correction, thereby improving the prognosis for VR. Therefore, ametropia must be properly corrected with glasses or contact lenses. Refractive errors correction alone is often enough to significantly improve functionality and is often the only prescription, especially in children.
Examination of refraction in patient with vision impairment does not differ significantly from the conventional method. Some difficulties are to be expected due to media opacities, changes in pupillary diameter, distorted images, nystagmus, or fixation problems1,3,9,10.
Retinoscopy is the gold standard for safe refraction1,2. Autorefraction is limited in low vision due to media opacities, the presence of nystagmus, existing high ametropias, or fixation problems19. Moving the patient closer for the examination can make the band sharper. Retinoscopy can be performed at a distance of 30 or 20 cm, and subtracting 3 D or 5 D, respectively, from the obtained value. When the retinoscopy exam is inconclusive or unfeasible, the determination of ametropia can be aided by keratometry, corneal topography, and axial length measurement and guided by the far/near VA values, if VA tables based on the minimum visual angle are used. Functional assessment, together with the likely ametropia, can guide the prescription. For VA up to 0.5, the crossed cylinder can be performed with a variation of 0.25. For worse VA, a variation of 0.5 is recommended, and for VA below 0.05, a variation of 1.00 D is recommended to allow better perception by the patient (Figure 6).
Dynamic and static retinoscopy are important for detecting manifest hyperopia and existing accommodation deficits, especially in children with neurological conditions.
Once the refractive error has been determined, VA is assessed under uncorrected and corrected conditions to verify whether the patient needs to be prescribed the same or a different correction. Far and near VA is also measured to verify equivalence between the two. If near VA is better, there may be residual uncorrected myopia, and if far VA is better, there may be uncorrected hyperopia. Near vision is tested with correction. For patients over 40 years of age, add +2.50 to take the measurement at 40 cm. Trial lens sets and frames are recommended, especially if there is nystagmus or abnormal head position; in addition, they allow assessing functionality and tolerability of the ametropia. The vertex distance should be corrected for ametropia above 10 D. It is also important to consider age, emmetropization, accommodation, ocular alignment, goals to be achieved, risk of amblyopia, and progressing myopia. One should be careful to ensure good near vision in children.
Correction of the existing refractive error is recommended if there is an improvement of one or two lines in the VA measurement, improvement in nystagmus or head position, or improvement in image quality and consequent improvement in functionality and in high ametropia (amblyogenic refractive error), even if there is no improvement in VA at first. In aphakia, high myopia and irregular astigmatism, contact lenses are appropriate for improving VA, VF, and depth of focus. Astigmatism greater than 2.00 D must be corrected to allow full use of accommodation during near activities. Caution is advised when prescribing bifocal or multifocal lenses in the presence of large VF defects and oculomotor dysfunctions. When prescribing a hand-held magnifier, the distance refractive error should be corrected. For stand magnifiers, the prescription should correct the near refractive error or existing hyperopia1,3,10.
VA should never be related solely to the underlying disease. A simple pair of glasses can transform the lives of millions of people. Therefore, one should always believe that refraction benefits the patient until shown otherwise (Faye)3.
4. Ophthalmic examination
Ophthalmic assessment in VR is an extension of the clinical treatment; therefore, a complete examination should be performed. It should include an external inspection, assessment of pupillary reflexes, evaluation of extrinsic motility, biomicroscopy, tonometry, and fundus examination. Based on this thorough examination, it is possible to determine whether the findings are consistent with the ophthalmologic condition, propose any necessary clinical and/or surgical treatment, and outline a VR strategy1,3,19.
VISUAL REHABILITATION STRATEGIES
In general, VR strategies based on the ophthalmic assessment include the following processes: recommending optical/electronic aids, training the patient in the use of the proposed aids by teaching effective usage and exploring all possible functionalities, prescribing, providing follow-up, and referring for Braille learning, replacement with audio-based aids, and orientation and mobility training. Training should also cover strategies for autonomy in activities of daily living, safety, and psychosocial well-being1,3,10,11.
The types of resources used are divided into optical (using a lens or an optical system positioned between the observer and the object), non-optical (modifying the environmental characteristics and the material to be observed by non-optical means), electronic (integrating optical systems for magnification on screens and computer resources), and non-visual (sound-based aids). The prescription should be based on the individual and their specific needs, grounded in real and achievable expectations (Figure 6)1,7,10,11.
In conclusion, the VR consultation involves planning interventions based on the patient's ophthalmic condition, as well as their needs, expectations, and other concerns. These interventions are not made empirically or randomly, but are based on a thorough ophthalmic assessment that considers the patient's clinical history, visual functions, needs, and preferences, conducted through empathetic and welcoming listening. The patient-centered approach is the essence of VR and aims to promote the best possible visual performance within the individual's actual conditions.
REFERENCES
1. Jackson ML, Virgili G, Shepherd JD, Di Nome MA, Fletcher DC, Kaleem MA, Lam LA, Lawrebce LM, Sunness JS, Riddering AT; American Academy of Ophthalmology Preferred Pratice Pattern Vision Rehabilitation Committee. Vision Rehabilitation Preferred Practice Pattern®. Ophthalmology. 2023;130(3):P271-P335.
2. World Health Organization, Italian National Reference Centre for Services and Research for the Prevention of Blindness and Rehabilitation of the Visually Impaired. International Standards for Vision Rehabilitation: report of the International Consensus Conference Rome, 9-12 December 2015 [internet]. Moasca: FGE Editore; 2017
3. Faye EE. Clinical Low Vision. 2a. Ed.Boston/Toronto: Little, Brow and Company.1984. p.529
4. Sampaio MW, Haddad MAO, Filho HAC, Siaulys MOC. Baixa Visão e Cegueira: Os caminhos para a reabilitação, a educação e a inclusão. Rio de Janeiro: Cultura Médica: Guanabara Koogan, 2010.
5. Mogk LG, Mogk M. Macular Degeneration. The Complete Guide to Saving and Maximizing Your Sight. New York, United States of America: Ballantine Books. 2003. p.455.
6. Vale TC, Fernandes LC, Caramelli P. Charles Bonnet syndrome: characteristics of its visual hallucinations and differential diagnosis. Arq. NeuroPsiquiatr. 2014;72(5):333-336.
7. Gilbert C. Epidemiologia em baixa visão. In: Veitzman S. Coleção de Manuais Básicos CBO: Visão subnormal. São Paulo: Cultura Médica; 2000. p.9-17.
8. Fernandes LC. Reabilitação Visual: o que é, como e quando ocorre. In: Kara-José N, Rodrigues NLV. Saúde Ocular e prevenção da cegueira. Rio de Janeiro: Cultura Médica, 2009. p.155-9 (Tema Oficial do XXXV Congresso Brasileiro de Oftalmologia).
9. Refratometria ocular e visão subnormal / Conselho Brasileiro de Oftalmologia; coordenador Milton Ruiz Alvez; - 4ed. – Rio de Janeiro: Cultura Médica, 2018.
10. Fletcher DC. Low Vision Rehabilitation: Caring for the Whole Person. Ed.Hong Kong by Fletcher DC;1999. 162 p.
11. Colenbrander A. Assessment of functional vision and its rehabilitation. Acta Ophthalmol. 2010;88(2):163–173.
12. Castro CTM, Kallie CS, Salomão SR. Elaboração e validação de tabela MNREAD para o idioma português. Arq Bras Oftalmol. 2005;68(6):777-83.
13. Colenbrander A, Fletcher DC. Ophthalmology Clinics of North América. Saunders Company, 1994; p.269.
14. Classificação Internacional de Funcionalidade, Incapacidade e Saúde. Centro Colaborador da Organização Mundial da Saúde para a Família de Classificações Internacionais, org. Coordenação de tradução: Cássia Maria Buchalla. – São Paulo: Editora da Universidade de São Paulo, 2003.
15. Schuchard RA. Preferred retinal loci and macular scotoma characteristics in patients with age-related macular degeneration. Can J Ophthalmol. 2005;40(3):303–12.
16. Sunness J S, Annan J E. Improvement of visual acuity by refraction in a low vision population. Ophthalmology. 2010;117(7):1442-1446.
17. Moya STF. Retinose pigmentaria e visão subnormal: adaptação aos auxílios ópticos para perto e correlação com funções visuais [tese]. Belo Horizonte: Universidade Federal de Minas Gerais; 2001.
18. Burton MJ, Ramke J, Marques AP, Bourne RRA, Congdon N, Jones I, et al. The Lancet Global Health Commission on Global Eye Health: Vision Beyond 2020. The Lancet Global Health. 2021;9(4):e489-e551.
19. DeCarlo DK, McGwin G Jr, Searcey K, Gao L, Snow M, Waterbor J, et al. Trial frame refraction versus autorefraction among new patients in a low-vision clinic. Invest Ophthalmol Vis Sci. 2013;54(1):19–24.
| AUTHO'S INFORMATION |
|
 |
» Julia Nogueira Marx Gonzaga http://lattes.cnpq.br/2418145755719704 http://orcid.org/0009-0003-6179-7068 |
 |
» Luciene Chaves Fernandes http://lattes.cnpq.br/7701719253016287 http://orcid.org/0000000203856651 |
Funding: The authors declare no funding.
Conflicts of interest: The authors declare no conflicts of interest.
Received on:
February 2, 2026.
Accepted on:
February 12, 2026.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket